Home /
Expert Answers /
Biology /
case-3-13-pts-an-18-day-old-female-was-brought-to-the-emergency-room-by-her-mother-who-stat-pa242
(Solved): Case 3. (13 pts) An 18-day-old female was brought to the Emergency Room by her mother, who stat ...
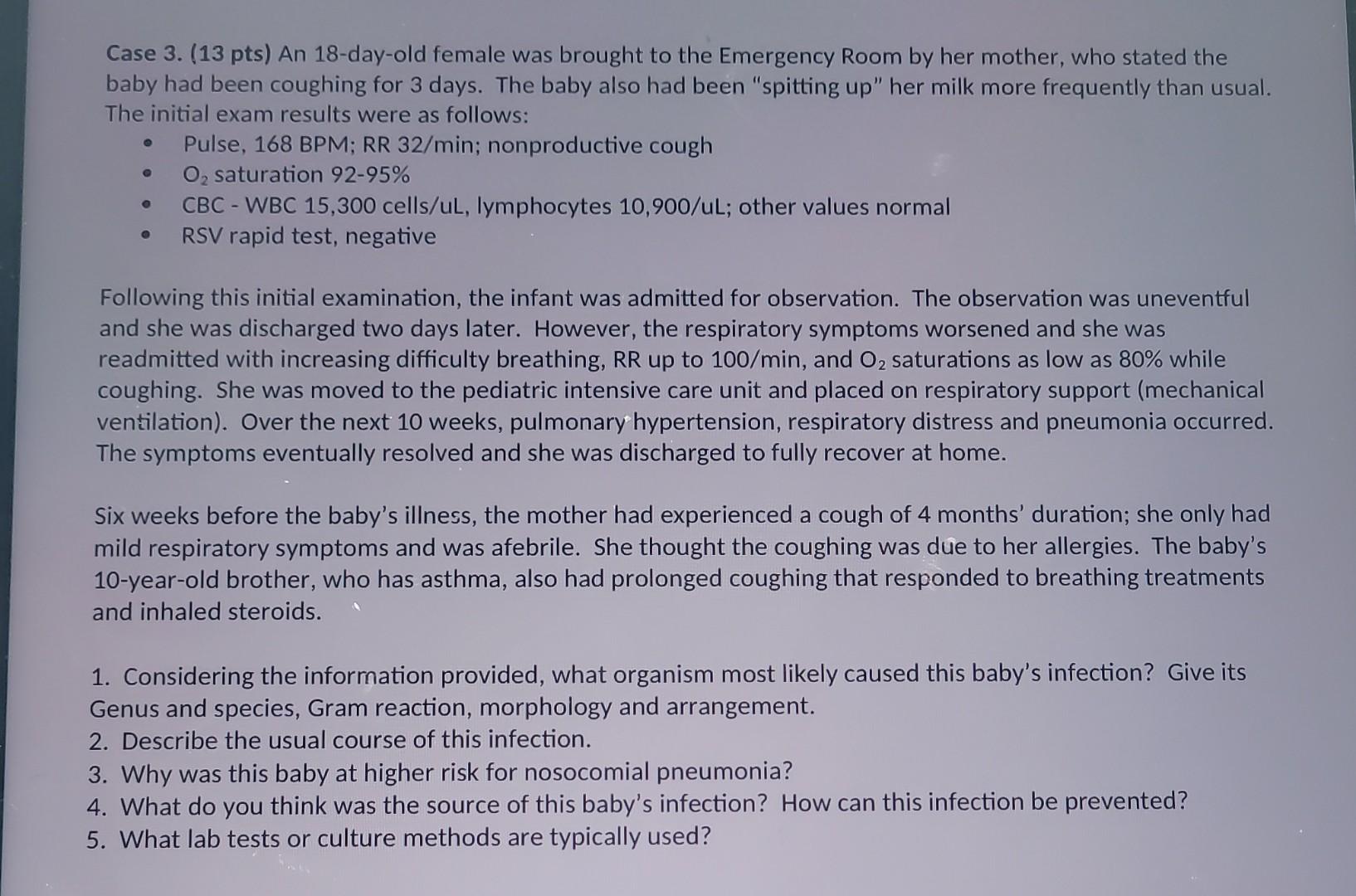
Case 3. (13 pts) An 18-day-old female was brought to the Emergency Room by her mother, who stated the baby had been coughing for 3 days. The baby also had been "spitting up" her milk more frequently than usual. The initial exam results were as follows: - Pulse, 168 BPM; RR 32/min; nonproductive cough - saturation - CBC - WBC 15,300 cells/uL, lymphocytes 10,900/uL; other values normal - RSV rapid test, negative Following this initial examination, the infant was admitted for observation. The observation was uneventful and she was discharged two days later. However, the respiratory symptoms worsened and she was readmitted with increasing difficulty breathing, up to , and saturations as low as while coughing. She was moved to the pediatric intensive care unit and placed on respiratory support (mechanical ventilation). Over the next 10 weeks, pulmonary hypertension, respiratory distress and pneumonia occurred. The symptoms eventually resolved and she was discharged to fully recover at home. Six weeks before the baby's illness, the mother had experienced a cough of 4 months' duration; she only had mild respiratory symptoms and was afebrile. She thought the coughing was due to her allergies. The baby's 10-year-old brother, who has asthma, also had prolonged coughing that responded to breathing treatments and inhaled steroids. 1. Considering the information provided, what organism most likely caused this baby's infection? Give its Genus and species, Gram reaction, morphology and arrangement. 2. Describe the usual course of this infection. 3. Why was this baby at higher risk for nosocomial pneumonia? 4. What do you think was the source of this baby's infection? How can this infection be prevented? 5. What lab tests or culture methods are typically used?
Expert Answer
Based on the information provided, I can provide general information about the possible causes and management of respiratory infections in infants.It